Monkeypox Business: one clear example why the WHO should never be trusted, especially by Africans
The WHO fear-mongering machine ramps up to poison the public with yet another MYOCARDITIS-inducing vaccine that probably does not work to prevent Monkeypox
… In the context of an outbreak, to allow the greatest flexibility for local risk assessment, varied modes of transmission and response options, the populations to consider for vaccination may include: (i) adults and children in a geographically defined area or community (e.g. villages) with a documented risk of exposure [not an actual exposure—what does risk of exposure actually mean?—Nass]; (ii) persons with multiple sexual contacts; (iii) health workers at risk of repe ated exposure; and (iv) known contacts of persons with mpox.
Noting the endemicity of disease in some African countries, the distinct epidemiology of mpox in these settings and the inequitable access to vaccination, SAGE issued a strong call to action to promote epidemiological and vaccine research on mpox in the African region and for urgent steps to facilitate equitable access to vaccination.
Research and systematic investigation and data collection should also be embedded in the outbreak response.
Final recommendations on vaccines and immunization for mpox will be published in May 2024
But here are the WHO’s data on Monkeypox published today, which they are counting on you not seeing:
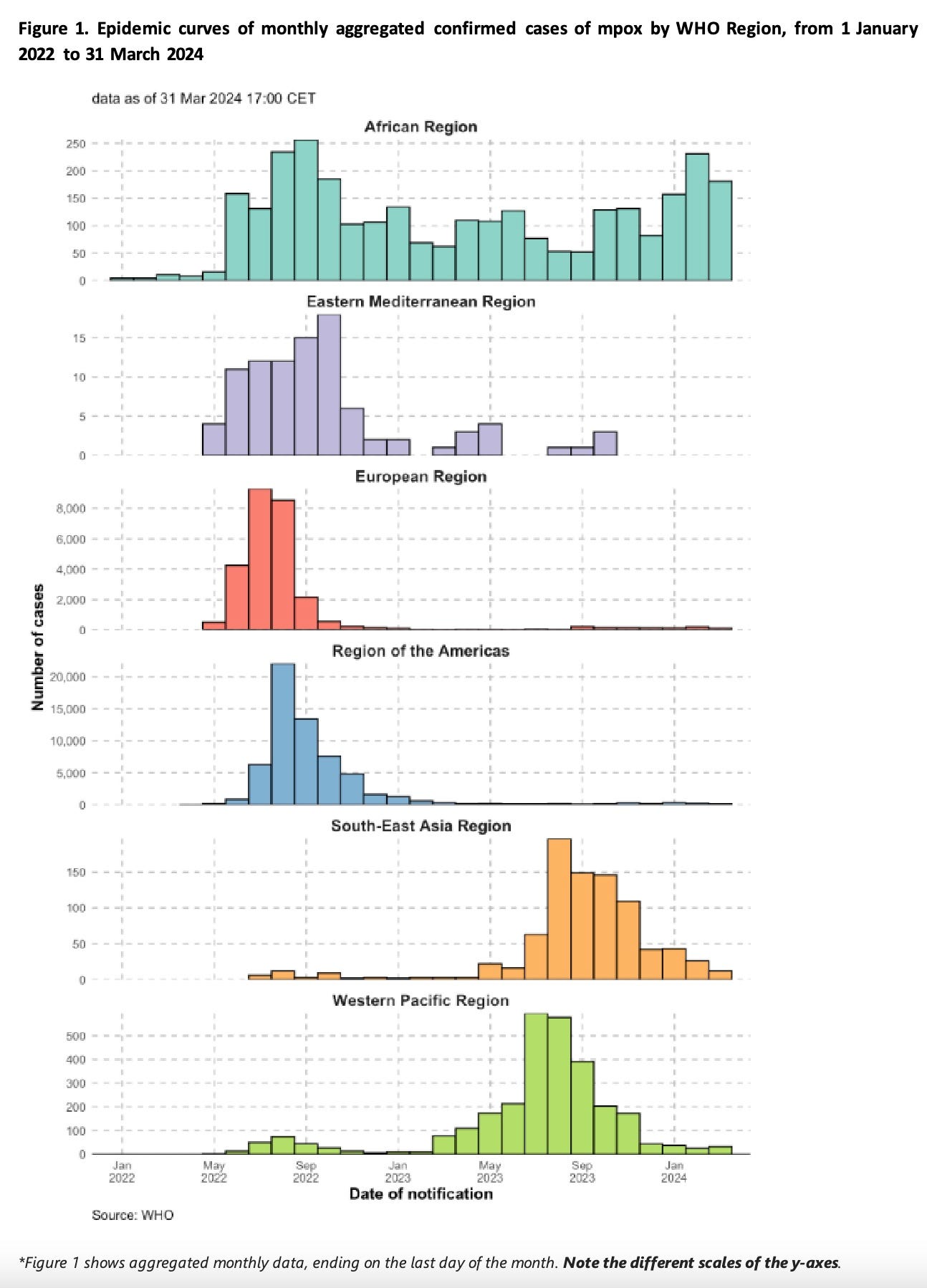
The only place cases are going up is Africa, which coincidentally is the easiest place in which the data can be faked.
The WHO reports that 185 people worldwide have died with monkeypox. The two I was able to obtain information on were critically ill before they got monkeypox. WHO says that 1 in 500 who had the disease died.
CDC has never reported efficacy and safety from the clinical trial it performed in the DRC between 2017 and 2020 on the Jynneos vaccine for monkeypox. I discussed this several times in this substack. There are other data that suggest the vaccine does not work. It failed to protect monkeys who were exposed experimentally.
FDA reports of the prelicensure clinical trials performed using Jynneos indicated that up to 10% or more of the subjects developed elevation of cardiac enzymes suggestive of myocarditis. The other vaccine used for monkeypox, ACAM2000, admittedly causes myocarditis. 1 in 175 recipients developed myocarditis from the vaccine according to CDC. Up to 1 in 30 had elevated cardiac enzymes according to research performed in US military servicemembers in the early 2000s by Renata Engler et al.
Bottom line:
-
Jynneos probably causes myocarditis but the rate is unknown and the long-term effects are unknown. We know little about other side effects.
-
Whether the vaccine actually works to prevent monkeypox and its actual efficacy, positive or negative, is unknown.
-
The reason this information is unknown is because a) FDA made sure to not collect the data after learning of the elevated cardiac enzymes, nor required additional information from the manufacturer, and b) CDC has hidden and in other cases misrepresented the data from its clinical trial in the DRC and other data gained.
-
Monkeypox is a mild, self-limited disease. We were told that 1-10% of cases would be fatal. The most WHO could come up with was a 0.2% fatality rate, which almost certainly reflects underlying diseases in cases.
-
Cases might be increasing in Africa but do not appear to be a problem anywhere else.
-
While “SAGE issued a strong call to action to promote epidemiological and vaccine research on mpox in the African region and for urgent steps to facilitate equitable access to vaccination,” this should be read as a recommendation to misuse the term equity to support experiments on Africans and to damage them for probably no benefit.