For the next two days, CDC’s ACIP will meet to discuss 11 vaccines. I will be commenting at this site from at least 8 am to 1:30 pm tomorrow
That is when the monkeypox, Lyme (experimental) flu and COVID vaccines will be discussed. Then I will comment on news from the WHO in Geneva.
The URL for the video changed and this is where they are broadcasting it from now:
https://www.youtube-nocookie.com/embed/dNCVr9AvFB8?rel=0&autoplay=0&showinfo=0&enablejsapi=0
The ACIP meeting has started and most of the voting members are new. They are almost all physicians at medical schools or health departments. As usual, CDC avoids showing us their faces.
Finally an official admission from CDC’s Dr. Minhaj that deaths from monkeypox have primarily been in patients with advanced HIV/AIDS.
Current recommendations for the 2 dose vaccine series are for those over 18 who are gay, bisexual, have sex with those people, or are promiscuous (defined as more than one sex partner, sex with sex workers, etc.). CDC guesstimates that 42% of “those eligible” got one dose and about 26% got 2 doses in 2022.
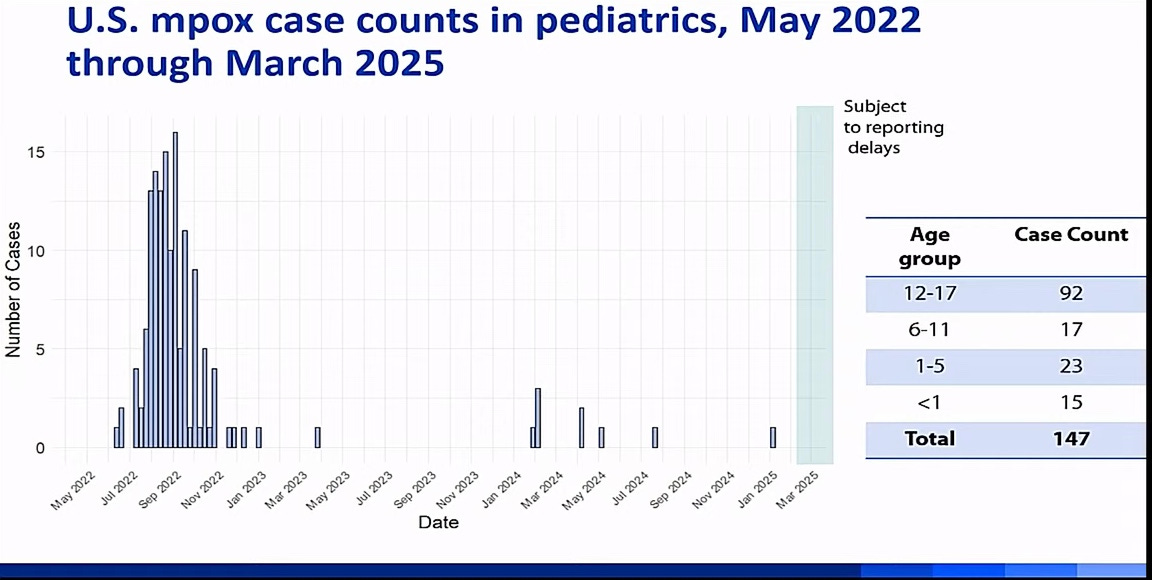
An NIH trial in 12-17 year olds (whose children were used?) was completed and the goal today is to extend the recommendation down to 12 year olds. It is unclear which CHILDREN would be at risk during an outbreak.
The work group chair is Prof Bonnie Maldonado, who worships at the shrine of vaccinology.
Dr. Buddy Creech of Vanderbilt U. presents on his NIH trial. He gets grants from NIH, CDC, Moderna and consults for Merck, GSK, Sanofi and other health companies. John Beigel of NIH was a member of the study team—he managed to perform misleading trials for COVID.
2 SQ doses 28 days apart in healthy 12-18 year olds to seek licensure in this age group. Recipients had a 7 day card to list symptoms. This was “our primary safety objective/ contributed to our safety objective.”
Through day 210 “we captured events including myocarditis” and through about a year we collected serious adverse events.
I hate that expression “out of an abundance of caution” which he used over and over to imply there were no real expected risks but we were the good guys being extra careful.
There were 315 adolescents and 211 adults and 6 were HIV positive. The most common systemic were myalgia (20-30%) and fatigue (30-40%). Overall, the adults reported more local reactions. There were many nodules at the site.
2 women became pregnant and the babies were normal.
1-2% declined a second dose. Geometric mean titres were low after the first dose but rose nicely after the second dose. Makes one question benefit of a single dose. There is no correlate of protection so these levels cannot be directly linked to protection. Since you can test lab animals it is hard to understand why there are no correlates of protection unless the reason is the vaccine does not work well.
He wants to get another grant to do a similar study in younger children. Of course.
I think it was Dr. Beigel who piped up that they have not gotten done “dissecting the mechanisms” by which the vaccine exerts its effects. I would note instead that they have not shown the vaccine works and are dancing around that uncomfortable fact.
Next talk with Pharm D Minhaj of CDC to discuss why the vaccine is so critical. CDC has a bogus process called Evidence to Recommendations Domains designed to convince us that vaccines are necessary, by calling in various forms of evidence that are sometimes irrelevant and by incorrectly weighting pieces of evidence. The purpose of this method is to minimize the importance of actual safety and efficacy and balance it with 5 other issues including the impressions of recipients and the impressions of primary care doctors (who may have never used it) about the vaccine.
Dr. Minhaj shows pictures of people with monkeypox and myocarditis, encephalitis and ocular infection. He tells us we may wish to avert our eyes from the next slide—monkeypox in the severely immunocompromised.
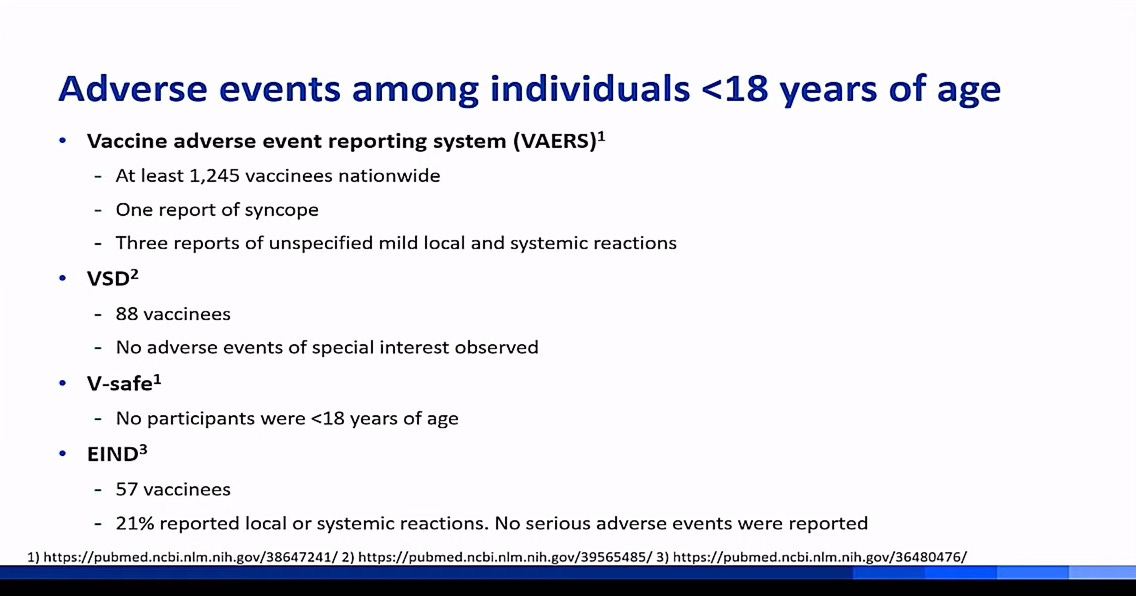
He says the vaccine was safe and well tolerated in adolescents. How did they monitor for myocarditis? It appears they failed to do so, even though it is the major concern for a serious adverse event. He says 4 major databases yielded any safety concerns whatsoever.
However, about 1 million Americans (almost all male) received this vaccine in 2022-2023; where are the results of the safety screening of this large population? MIA.
here is an example of taxpayer funding waste. over 500 mothers were surveyed to whether they thought their small children were at risk for monkeypox. Then they were asked if they thought the vaccine worked and of course most did. This was interpreted as support for the vaccine. By the end of the survey most mothers would be willing to vaccinate their children (most under age 10) at some point. DUH! I wonder if the purpose of this survey was to assess the best language to convince moms to go along?
Blacks get vaccinated less than whites in the US. This is considered a problem of equity rather than a considered choice. Given the assumption that poor blacks must therefore lack access to vaccines, efforts are discussed to make it easier to vaccinate them. When will CDC acknowledge how paternalistic and hypocritical they are?
Jynneos vaccine is licensed and people will have to pay for it but the cost is never mentioned, of course.
Here are some relevant slides. Note that the MPOX photos are now accurate, whereas before we were often looking at old smallpox or zoster slides. Note that there are few US cases in children—about 10 in a year.

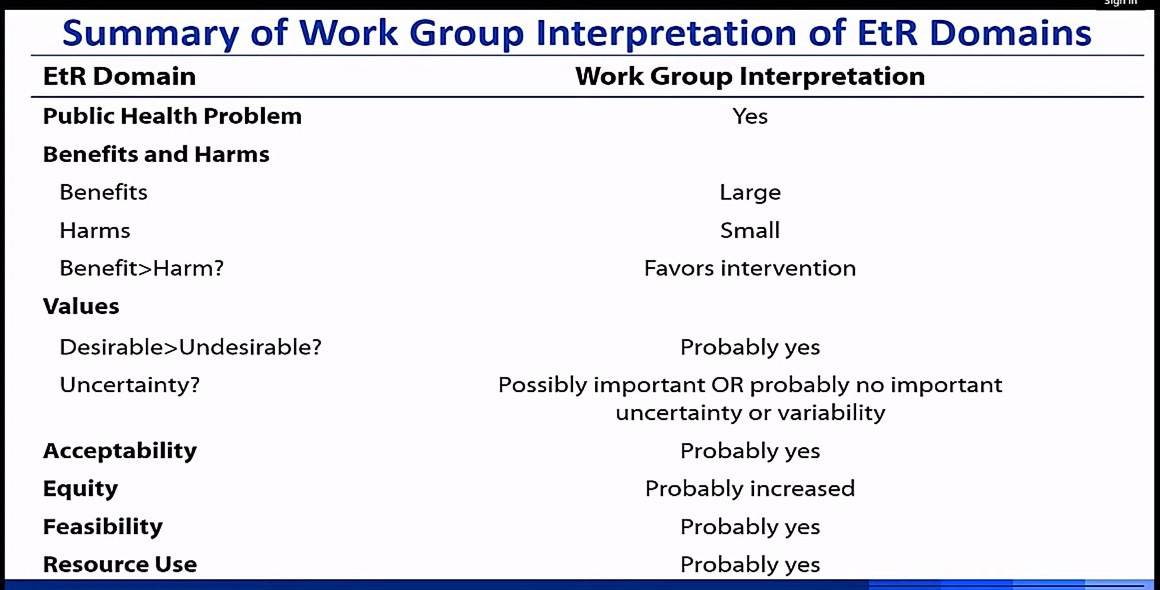
Above you can see the 7 Domains that are irrelevant to a determination of whether to license this questionably safe and effective vaccine for children who don’t need it—as I said, this method was chosen to minimize the important of making a decision based only on safety, efficacy and necessity. Acceptability, equity, feasibility, resource use are bogus considerations that are only included to allow the ACIP to support every vaccine, even when it has a poor risk-benefit ratio. Benefits and harms has been reduced to only one of seven issues to be considered by these “experts” who allow themselves to be treated like children by participating in this charade.
I would suggest that the EtR method be quickly disposed of.
Creech was asked how they evaluated myocarditis. He said nothing generated the need for such assessment, it does not seem to happen in adolescents. Buddy, you also tested over 200 adults, remember? But the unpublished licensure data I reviewed on CDC’s website showed that military service members had elevation of troponin in as many as 10% and 18% in different studies—they are close to the age of adolescents, and we know for COVID the 12-17 year age group is at higher risk of myocarditis than other age groups.
BTW if you want to watch the broadcast is here:
https://www.youtube-nocookie.com/embed/RR7Es9sdNpY?rel=0&autoplay=0&showinfo=0&enablejsapi=0
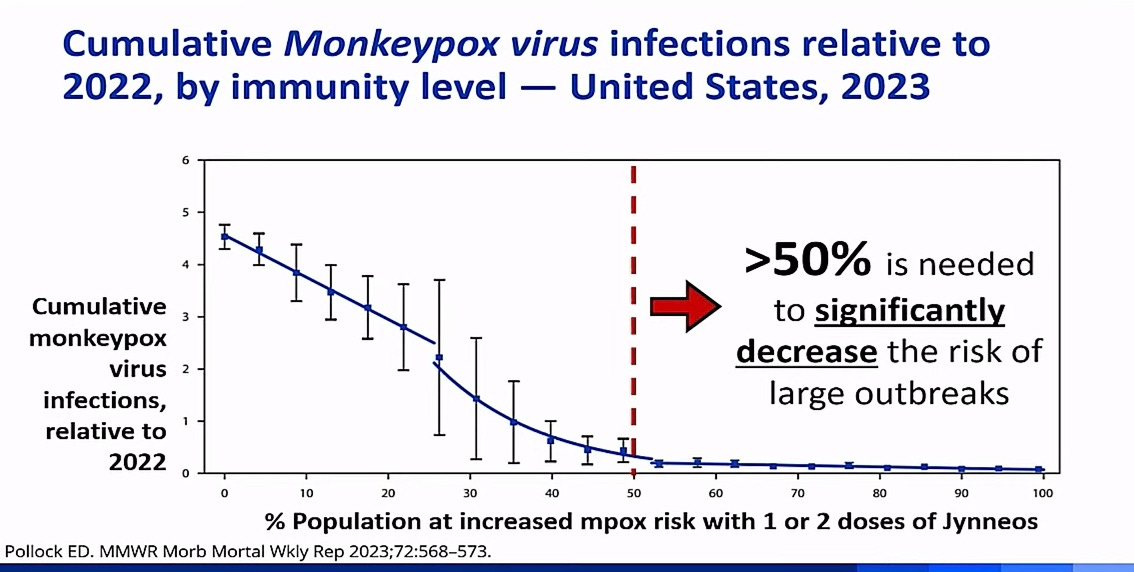
Earlier it was stated that if under 50% of at risk people are unvaccinated there could be more infections, rather than less. This slide supposedly reveals this. I don’t get it.
By choosing to look only at a few adverse events and ignoring the 1.2 million doses that were given experimentally, which means the USG was obligated to collect adverse event data on them, the CDC is enabled to make the claim that the vaccine is safe.
The CDC tried to fool the committee regarding Resource Use. Jamie Loehr pointed out there were only 10 adolescent cases in the US in 2 years —we don’t know the vaccine price, there are a very small number at risk, and so it is fishy that CDC claims they lacked data to make an assessment of resource use, so they let it slide. CDC tries to distract by making this about HIV Prep treatment.
Tracy Beth Hoeg MD PhD assistant to Dr. Makary makes an announcement that there were few cases, little safety data—it is very challenging to claim the benefits outweighs the harms. Adolescents with underlying diseases were excluded from the trial. Yay! Somehow who represents sanity and the new administration is at the table!!!
CDC does its usual handwaving in response.
There will be a short break because of a technical issue and there will be a new link on YouTube, posted on the current link.
Naturally CDC did not make it easy to find the next URL, which is this:
https://www.youtube-nocookie.com/embed/dNCVr9AvFB8?rel=0&autoplay=0&showinfo=0&enablejsapi=0
I missed Lyme disease, which was just a short announcement.
The California data on flu vaccine efficacy are being presented, presumably in order to challenge the Sresthra Cleveland Clinic data that showed 27% negative efficacy.
The CDC data claims that the flu shots actually had about 50% POSITIVE efficacy—in other words, a disagreement of about 75%. Massive disagreement. Let me show you the slides.
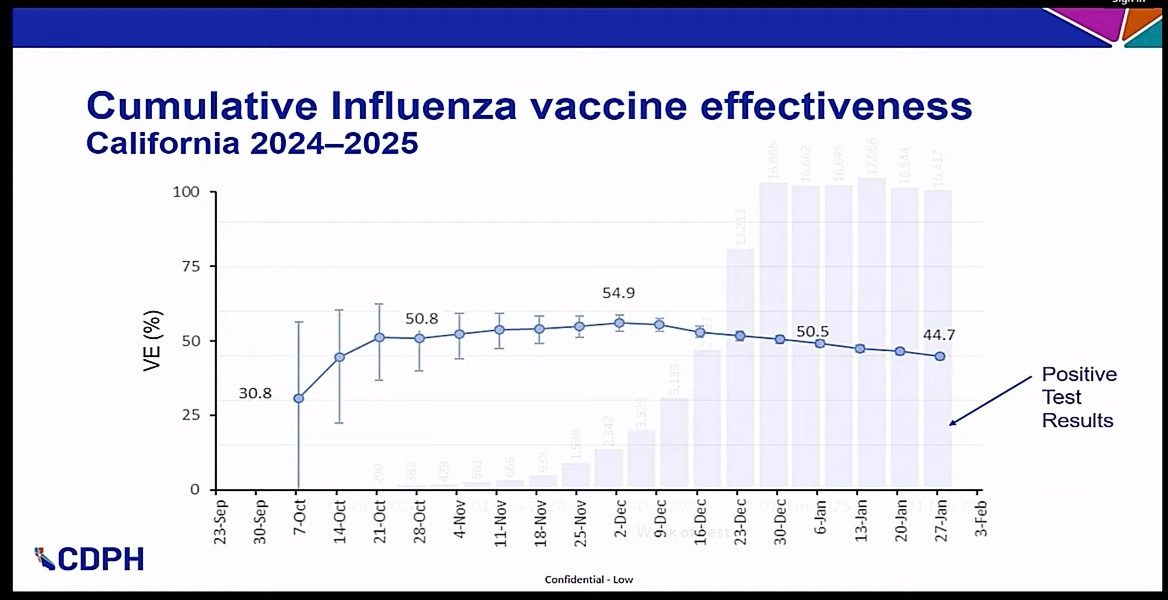
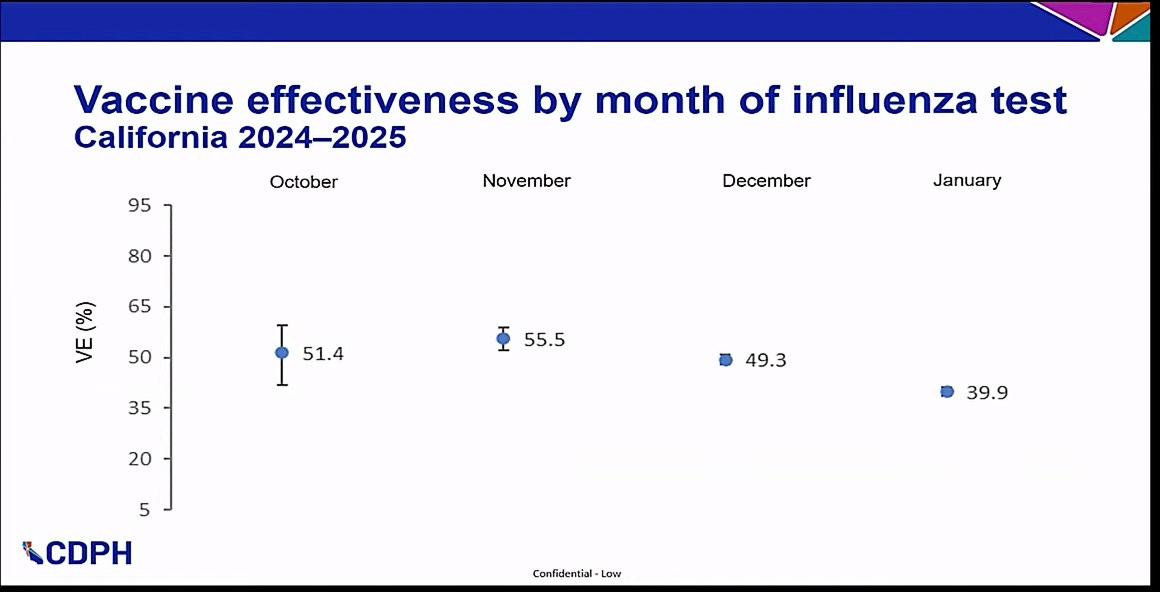
Dr. Asturias wonders if the above 15.6% drop in efficacy from November to January is due to very short period of efficacy, and asks about the dates of vaccination. CDC staff hand wave and do not provide the requested data, but suspect it does wear off quickly. Maybe people should be vaccinated later? This is an old issue which CDC ignored when it moved vaccinations to August and September to get more vaccinations in. This is important because most flu occurs in Jan-Feb, and it is said to take up to 1 month to maximize immunity after a shot.
I have heard no one has mentioned the Cleveland Clinic study and why these data are so very different. Of course. Unless I missed it, but I don’t think I did.
Oops, got to go meet my tax accountant and will have to miss this boring meeting for several hours.
Back at 1 pm. The ACIP workgroup wanted a “risk-based” recommendation for COVID shots and the professional organizations like ACOG and AAP agreed with this.
The current speaker claims COVID remains a major cause of death in adults and children. Really? She wants a universal, yearly flu and COVID recommendation: yearly shots for everyone. De Loehr says covid is serious and common. Dr. Brooks is concerned about long covid coming from the infection, not the vaccine, and uses this as a reason to vaccinate.
Attending these meetings is like entering an alternate universe in which the ACIP members and CDC staffers are deaf and blind to any comments anywhere that are negative about vaccines. It is hard to believe they don’t see injured patients.
I think it was Dr Hoeg who asked about how Moderna could assess its current covid vax efficacy when it had not established the efficacy of the baseline vaccine against which it was being prepared. The Moderna briefer tried twice to answer a different question when Tracy Hoeg repeated the question. Then his boss stepped in and simply claimed they do measure efficacy. He failed to say how, where to find the data, nor what the results were. End of conversation. Now it is time for the lunch break.