A few remarks on the 6/25-6/26 ACIP meeting, thimerosal and a primer on chikungunya
Don't worry, I can neither pronounce nor spell it, either
A new Advisory Committee on Immunization Practices group of 7 was seated and asked to deliberate on many vaccine issues. I did my live blog, and while making snide comments from time to time allows me to let off steam, watching these meetings really takes the wind out of my sails. I can see how some CDC staffers set up the committee to fail. I can see how the process creates its own biases. And it was obvious that the new members, unfamiliar with the complex processes at play, felt they had to go along to get along, at least while they gain familiarity with what they can say and do that is within the realm of acceptability.
While it seemed that some issues would be a slam dunk, they weren’t. Whether there was still a place for neurotoxic (ethyl) mercury in vaccines turned out to be controversial. More than one person complained that the committee was wasting time even discussing the question. After Lyn Redwood gave an excellent overview of the role of thimerosal (50% ethyl mercury by weight, previously known as merthiolate), it was revealed it really was not such a good antiseptic, and that multidose vials were not even a necessity. Most Americans were receiving flu shots from single dose vials without thimerosal, or maybe there was just a little bit in those vials.
Should a new RSV monoclonal antibody (about which the committee received only the most cursory of briefings) be added to the Vaccines for Children (VFC) Program? When members hesitated, Dr. Meissner pointed out that this was an issue of equity. Poor kids without insurance needed to access this monoclonal antibody too. Immediately, everyone voted yes.
50% of US kids get their vaccines for free through the Vaccines for Children program, initiated by Bill Clinton.
According to Google, “multi-dose presentations of Afluria, Fluzone, and Flucelvax can contain thimerosal. However, single-dose presentations of these vaccines do not contain thimerosal.”
However, CDC waffles on this: “Flu vaccines in multi-dose vials contain thimerosal to safeguard against contamination of the vial. Most single-dose vials and pre-filled syringes of flu shot and the nasal spray flu vaccine do not contain a preservative because they are intended to be used once.”
And by the way, why did it take FDA 4 years to remove a flu strain from the flu shots after it stopped circulating? Did they have to help big Pharma use up its stash?
Beginning with the 2024-2025 flu season, the influenza B/Yamagata vaccine component in U.S. flu vaccines is being removed because influenza B/Yamagata viruses have not been detected by global flu surveillance after March 2020. Because B/Yamagata viruses are not actively circulating in people, the risk of infection with B/Yamagata lineage viruses is considered to be low at this time. A variety of data and criteria were used to make the vaccine recommendations.
The risk is not low, it is zero.
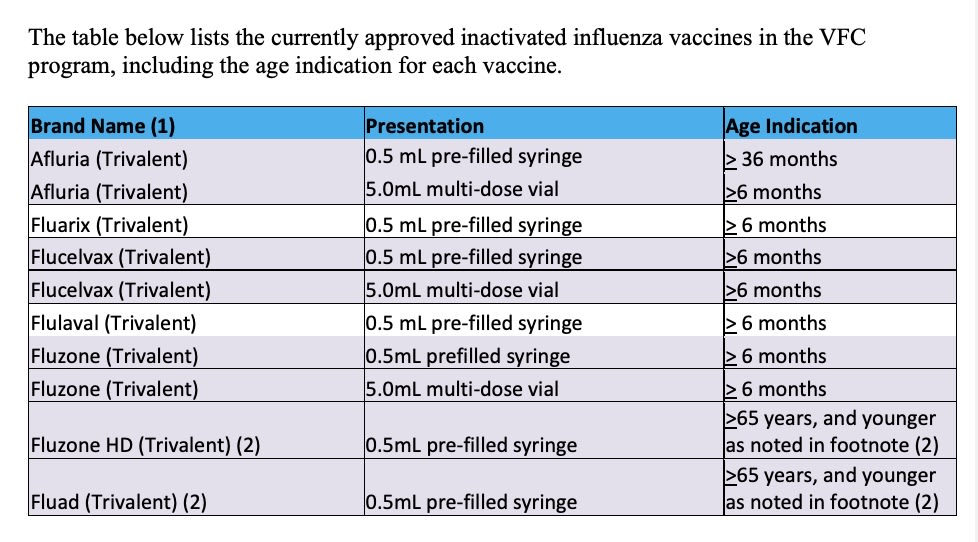
Which vaccines are approved for this federal VFC program for uninsured kids, Native Americans and the like? Here is the list, and by golly, all the vaccines that come in multidose vials with thimerosal are on the list. What happened to equity in this case? It appears that when the government is buying, you are more likely to get a thimerosal-containing vaccine, and it is less likely when you are buying.
Too many people today claimed that thimerosal had not been absolutely proven to cause harm to infants, so it was okay to keep jabbing them with a proven neurotoxin. When did medicine scuttle the Precautionary Principle? Quite a while ago, it seems.
Chikungunya. Why did the ACIP have to spend time on this vaccine today? There are two Chikungunya vaccines available, it seems, licensed since 2023. There was no scheduled vote. We have heard about these vaccines at ACIP meetings multiple times over the past 3 years. Is Chikungunya a big problem?
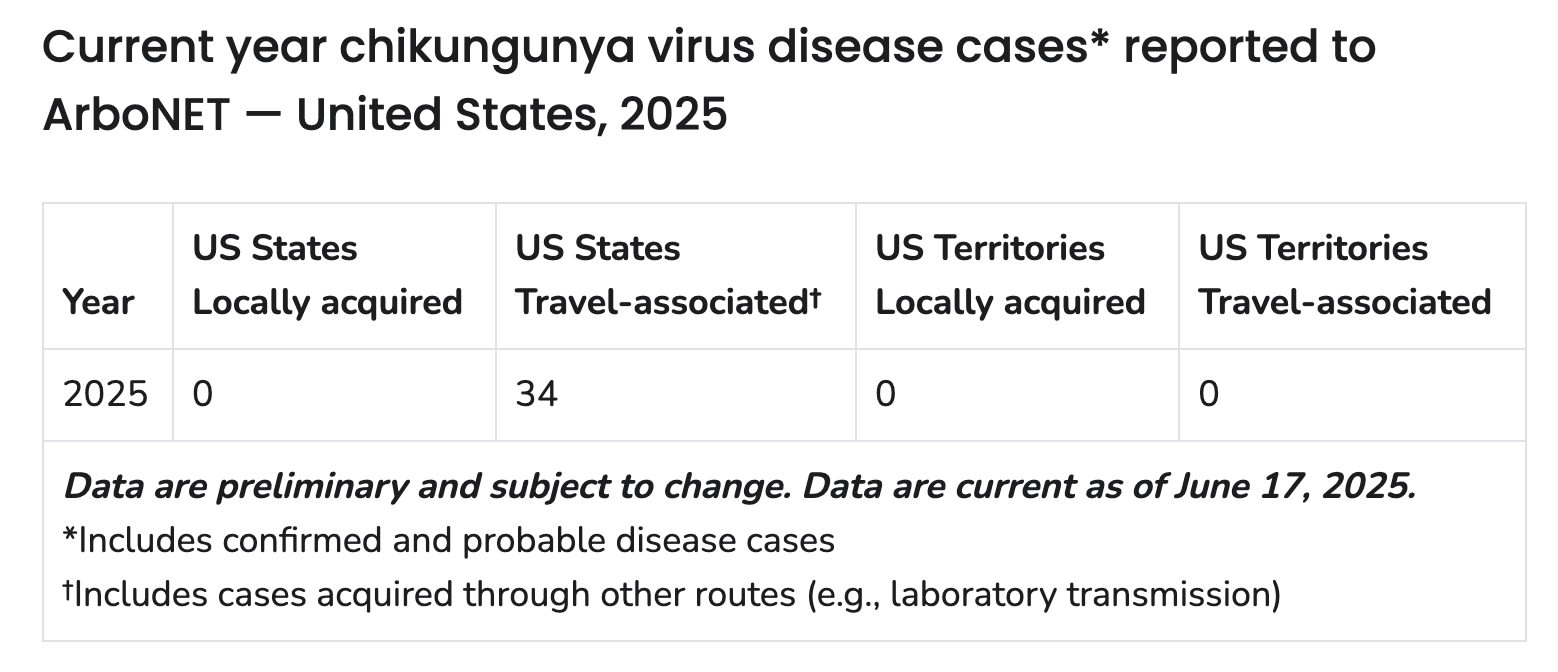
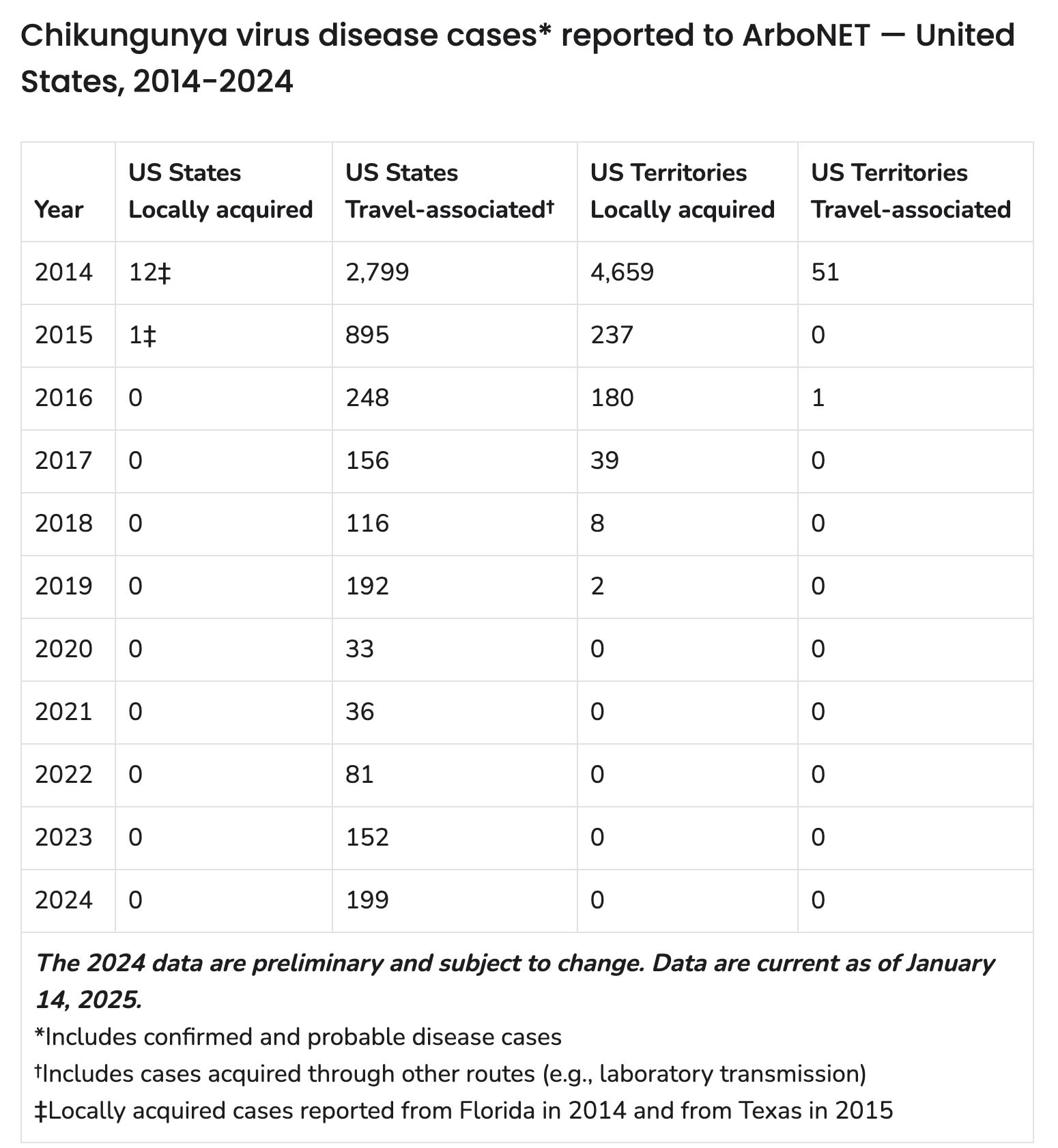
Nope. Here’s the history. Read the last bullet point.
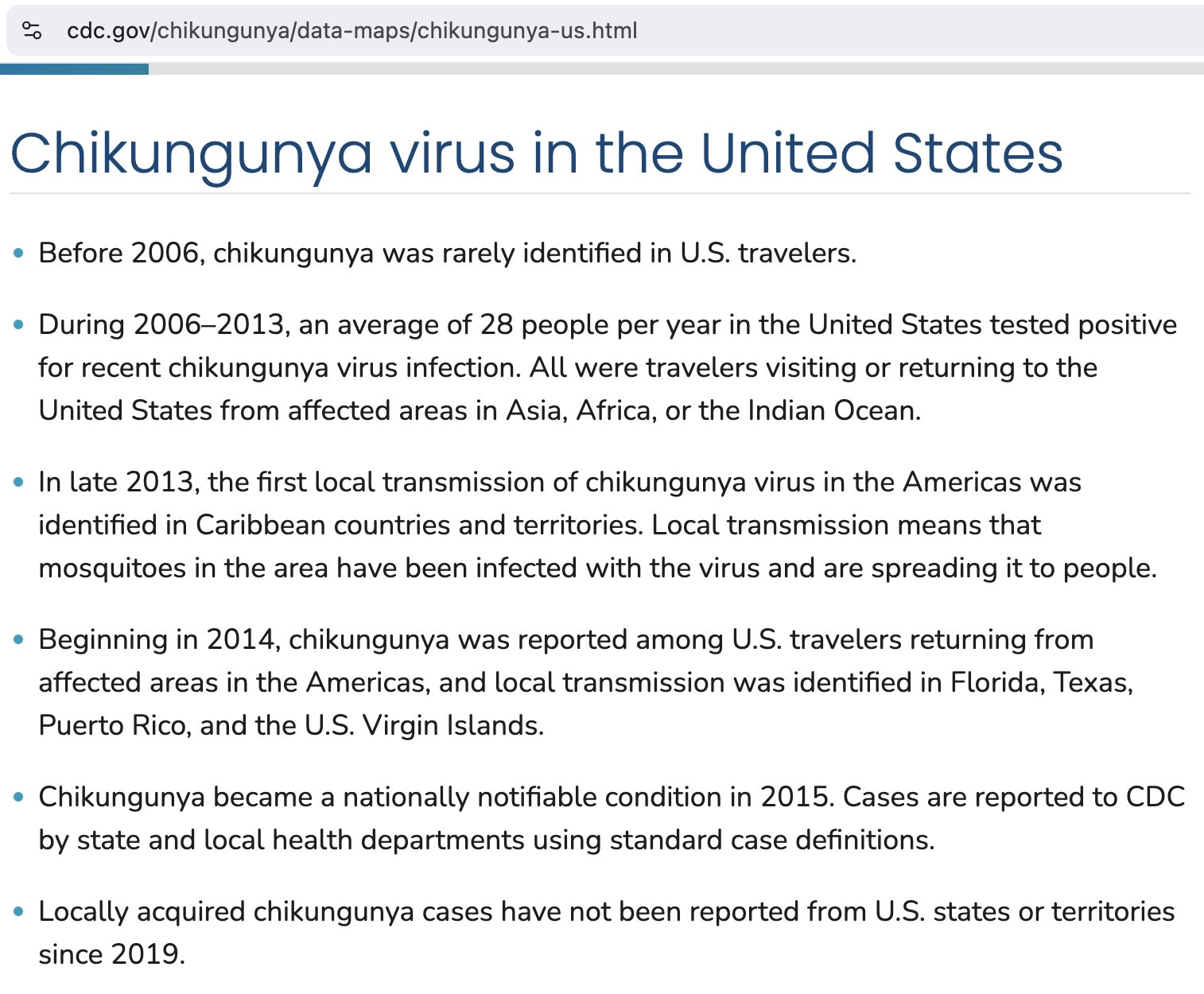
This year, there has not been a single case reported, not in the Virgin Islands, Guam, Hawaii, Puerto Rico, Texas. Not only that, there has not been a single case acquired in any US state or territory since 2019.
So why did we need 2 vaccines? Or one? Because biotech needs ever expanding markets. And FDA is a pay to play institution now, gaining approximately 50% of its budget from “user fees.” FDA is a mill, and drug/vaccine applications are its grist.
Well, when the first chikungunya vaccine was presented to ACIP, the briefer claimed the disease was associated with a high mortality rate. So I looked it up during the meeting and found that was untrue. After that, CDC briefers focused on it causing joint pain that could be prolonged. Of course, since this is a mosquito-borne disease, the safe way to handle it is with insect repellant and/or permethrin-treated clothing. And now there have been serious complications in those over the age of 60 from the vaccine, so it has been paused in Europe in that age group, and in the US as well. Thing is, you have no need of it. Do NOT be an early adopter. The other name for early adopter is guinea pig.
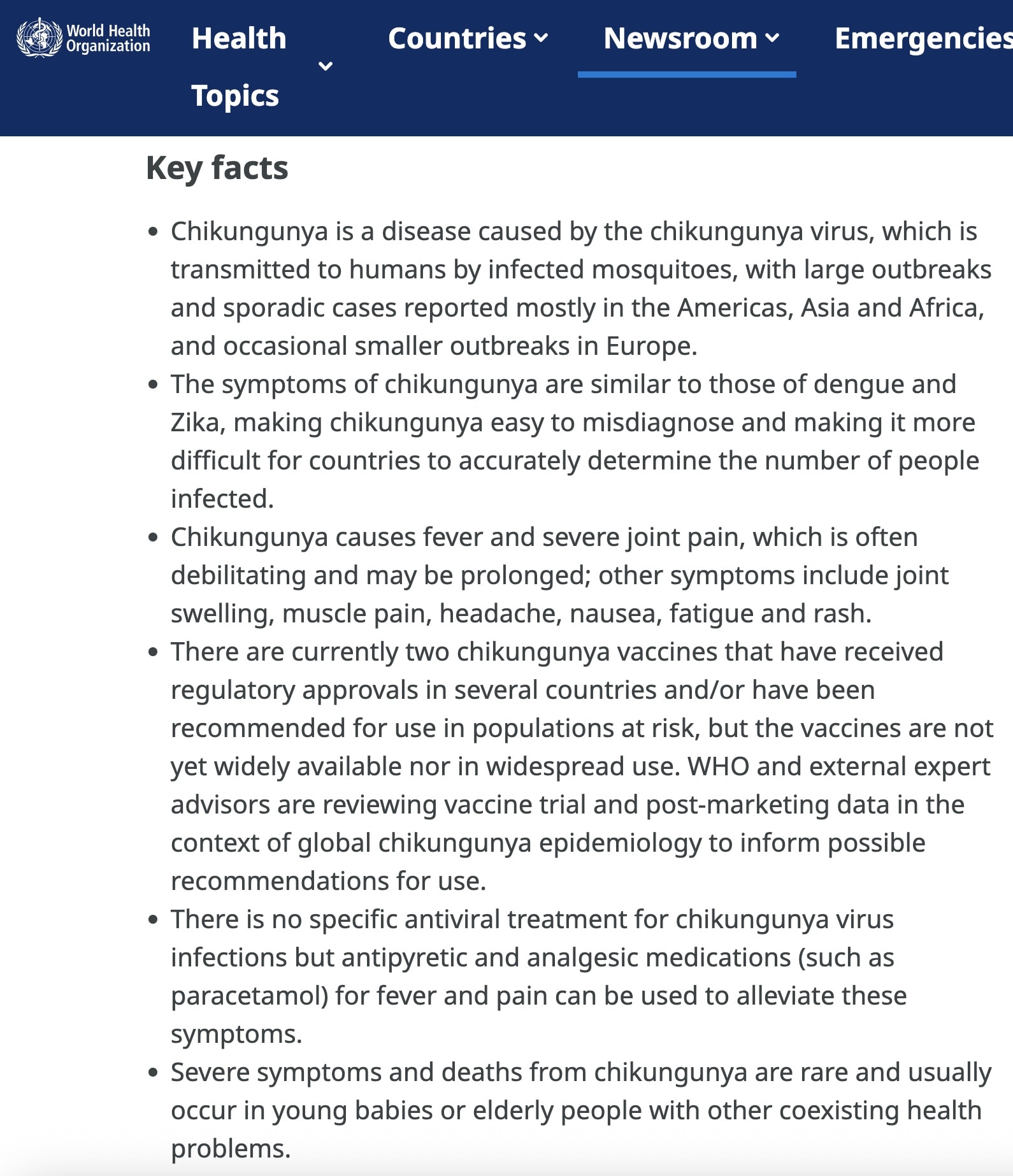
Here is the truth about the disease. The symptoms are similar to dengue or zika. Unpleasant, but it only rarely causes persistent symptoms. Use bug spray if you travel to an area with Chikungunya and call it good.
And then ask why it was claimed that a discussion of thimerosal wastes the ACIP’s time, but a discussion of chikungunya vaccines does not.
Maybe if we actually started looking for treatments for viral diseases like chikungunya we would find generic drugs that worked. But that would be a disaster for the biotech industry.
https://www.who.int/news-room/fact-sheets/detail/chikungunya