If you want good protection against meningitis and seek a Penbraya (5 valent vaccine) or other meningococcal vaccine, THINK AGAIN. Learn the real facts on meningococcal meningitis.
If you want good protection against meningitis and seek a Penbraya (5 valent vaccine) or other meningococcal vaccine, THINK AGAIN. Learn the real facts on meningococcal meningitis.
The protection is uncertain and the duration of uncertain protection is very short.

First, we have the GAVI propaganda to go get your shot. The UK is having an outbreak OF MENINGITIS B with about 20 cases—which is enough to urge millions OR BILLIONS to get jabbed.
Here is what you need to know:
-
Meningitis (meningococcal meningitis, which is the only type of meningitis the shots are intended for) is a bacterial disease that readily responds to antibiotics. Early treatment will knock it out without a shot. But you need to know the signs and symptoms, which I will list below, to take the antibiotics quickly.
-
Between 1% and 25% of the public harbors the bacteria that cause this form of meningitis (Neisseria meningitidis) in their noses and throats virtually all the time—and neither they nor their close contacts catch the disease. No one understands this.
-
This may actually be protective, causing those who harbor the bacteria to be immune.
-
The disease, when it does occur, progresses rapidly within hours and can be deadly or disabling. But it is very very rare. Less than 300 cases per year in the US—less than one case per million Americans yearly.
According to the CDC:
N. meningitidis was identified in 329 (6.5%) cases of meningitis. Between 2008–2009 and 2010–2019, the overall incidence of N. meningitidis meningitis declined by 66.5% (95% CI: −73.9, −56.8) from 0.19 to 0.07 per 100,000 (Table 1). Between 2010–2019 and 2020–2021, incidence declined by 53.9% (95% CI: −71.5, −29.4) to 0.03 per 100,000. [About 100 cases per year in the US—Nass] There was no change in incidence between 2020–2021 and 2022–2023. Overall, 299 (90.9%) isolates were serogrouped. Declines in N. meningitidis meningitis case counts were observed across all serogroups over time. However, there were changes in serogroup proportions; notably, the proportion of N. meningitidis serogroup Y isolates increased from 7.2% (5/69) in 2015–2019 to 36.8% (7/19) in 2020–2021, and 39.1% (9/23) in 2022–2023 (Appendix 7).
-
Symptoms include (memorize these):
-
Fever
-
Stiff neck—this is key
-
Sensitivity to light (photophobia)
-
Headache
-
Confusion, irritability or other altered mental status
-
Lack of energy, extreme sleepiness
How are meningococcal meningitis outbreaks defined, and who should be treated with a jab or a pill when there is an outbreak in your neighborhood?
For meningitis B, you only need 2 cases within 3 months to call it an outbreak and start offering (or requiring) shots. But the shots take plenty of time to work (about a month) so antibiotic pills are a much better answer, as they work immediately.
The vast majority of meningococcal cases, according to CDC, are not associated with outbreaks and occur out of the blue. Only 5% of cases were associated with outbreaks from 2009-2013!
Outbreak-associated cases account for approximately 5% of all meningococcal disease cases in the United States. Serogroup B is the primary cause of organization-based outbreaks, with the majority of university outbreaks due to serogroup B, and serogroup C is the primary cause of community-based outbreaks.
In other words, despite receiving multiple doses, the protection does not last very long. The Men B part of the vaccine requires boosters every 2-3 years, while they say the other components last about 5 years. But who knows? Disease incidence began decreasing long before the vaccines entered general use, so how effective they are is uncertain.
Why would you take a vaccine for an extremely rare disease that can be effectively treated with antibiotics but requires extremely frequent boosters?
Isn’t it likely that any vaccine benefit will be outweighed by vaccine side effects?
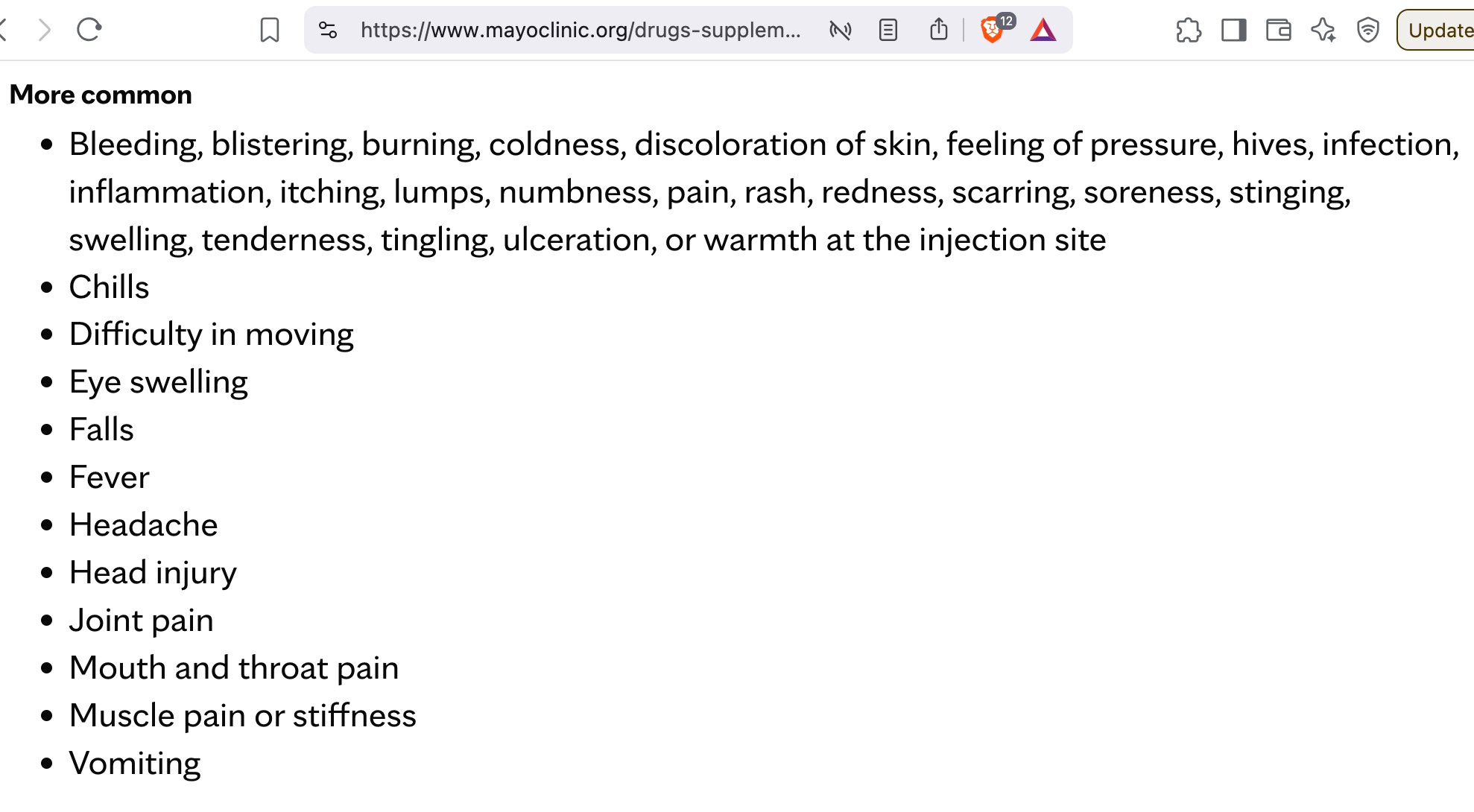
And sure enough, the vaccine can cause the paralytic Guillain-Barre syndrome, which can disable or kill you. What does the Mayo Clinic say about the side effects of the meninogococcal vaccines?
If I ruled American public health, I would give every American a meningitis symptom list, one or two doses of rifampin to hold onto and take at first sign of meningitis (assuming no allergy—allergy is extremely rare to this antibiotic), (all this in lieu of the shot) and a phone number to get immediate care (say via ambulance) for suspected meningitis, or to speak to a doctor to discuss whether to take the pills. You would have much better outcomes and fewer serious adverse effects this way.