Day 3 of the CDC (Centers for Disinformation, Criminality and Prevarication) Advisory Committee on Immunization Practices meeting
I didn’t want to dive down into the CDC sewer for a second time today
and recreate today’s ACIP meeting so I could write it up. But then I
realized I really have to come to grips with the fact that our culture
has spawned a bumper crop of Stepford wives/lemmings/robotic gibberish
producers and we have to figure out how to bring them back to life or at
least reprogram them so they are good for something. I hope to write
more on that large topic later.
The mission of CDC and the ACIP
members is to sign off on all possible vaccines as safe and effective,
and to never turn over any stones that could reveal anything different.
Then to roll all vaccines out to as broad a group of humans as humanly
possible.
To that end, the ACIP members are presented with bits of
partial information. They never ask for more. And everyone speaks in
code, which is why I started watching the meetings, because they are
hard for normal people to understand, and I felt they needed a
translator.
Today’s meeting began with Monkeypox vaccines. There are two, because both were intended for smallpox. ACAM2000
was purchased starting 25 years ago and after the anthrax letters a
dose was bought for every American—after the old smallpox vaccine that
was stored frozen for decades was destroyed, allegedly to save money on
electricity.
Let me remind you that monkeypox is
essentially like shingles. CDC tried to make it seem serious with some
gruesome photos today, then admitted they were of end-stage AIDS
patients with monkeypox too. It is a mild disease and there is no need
for a vaccine for 99.9% of people; and if you get it you will probably
have real immunity afterwards.

ACAM2000
was assumed to be safer than the older (NYC Board of Health brand)
vaccine, but it turned out it wasn’t. It caused myocarditis and it
could spread from the inoculation site to other people, just like the
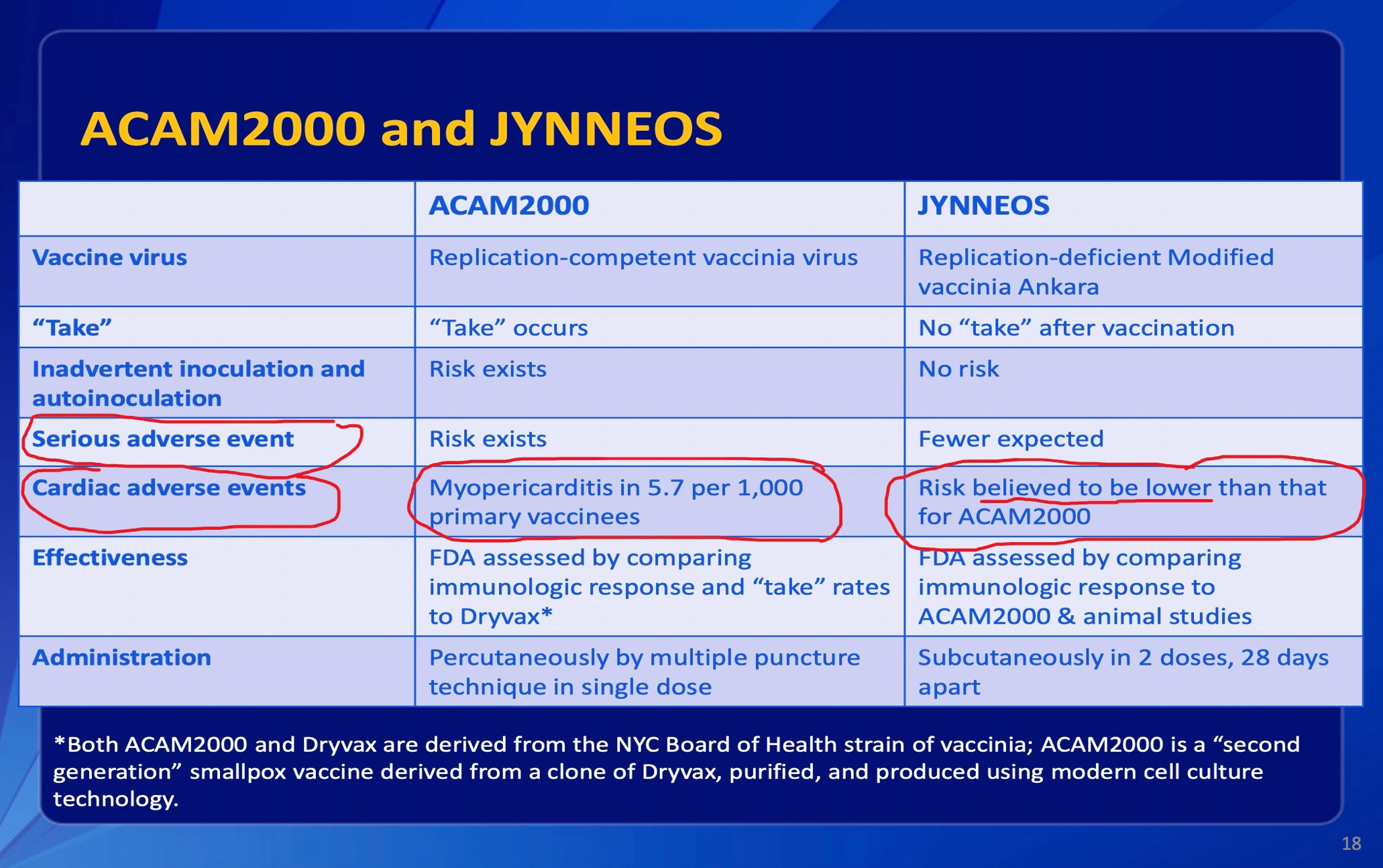
old vaccine. Last year CDC said ACAM2000 caused
myocarditis in 1 in every 175 recipients who were not previously
vaccinated for smallpox. That is a very huge, disastrous side effect
profile, but it didn’t stop the military giving the vaccine to most
soldiers. Here is CDC’s own slide with my red pen:
So
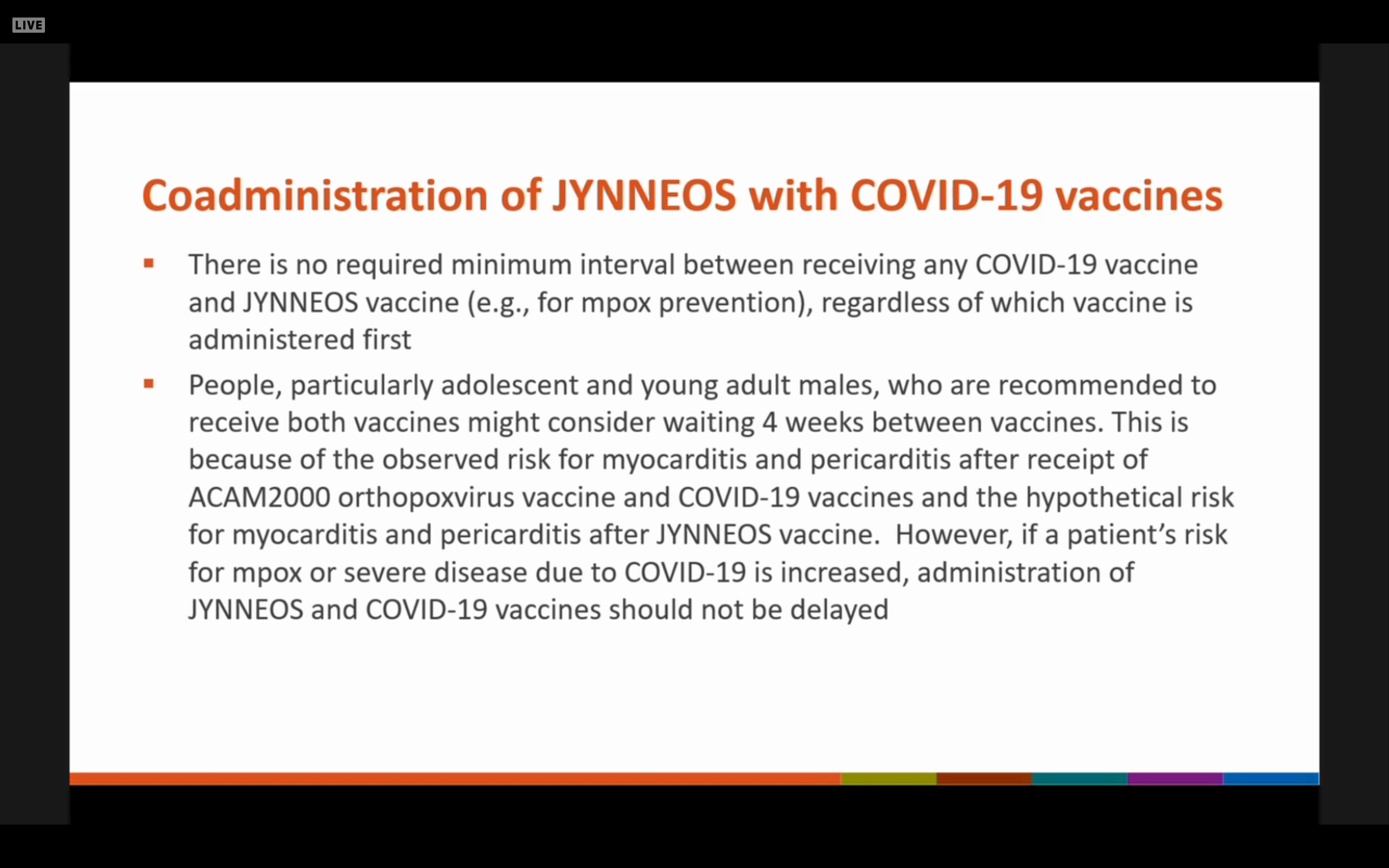
the USG went with Jynneos, guessing it was safer. And CDC is willing
to give it along with COVID vaccines, even though that probably
magnifies the risk of myocarditis.
Perhaps
it is safer. However, the human trials that looked at cardiac enzyme
levels found a lot of elevations (10% and 18% of subjects in two small
trials) which the manufacturer, the US military (it was tested in
soldiers) and the FDA chose to avoid investigating further.
The officials are blame averse. Irresponsible. They do not take care of the people whose safety they are charged with protecting.
Working for the government, they have a pension to protect. The
manufacturer has only one customer, the USG, and the customer wanted any
problems ignored or hidden. After throwing $2 Billion at Jynneos over
20 years there simply could not be any problems. This is just one recent contract of several:

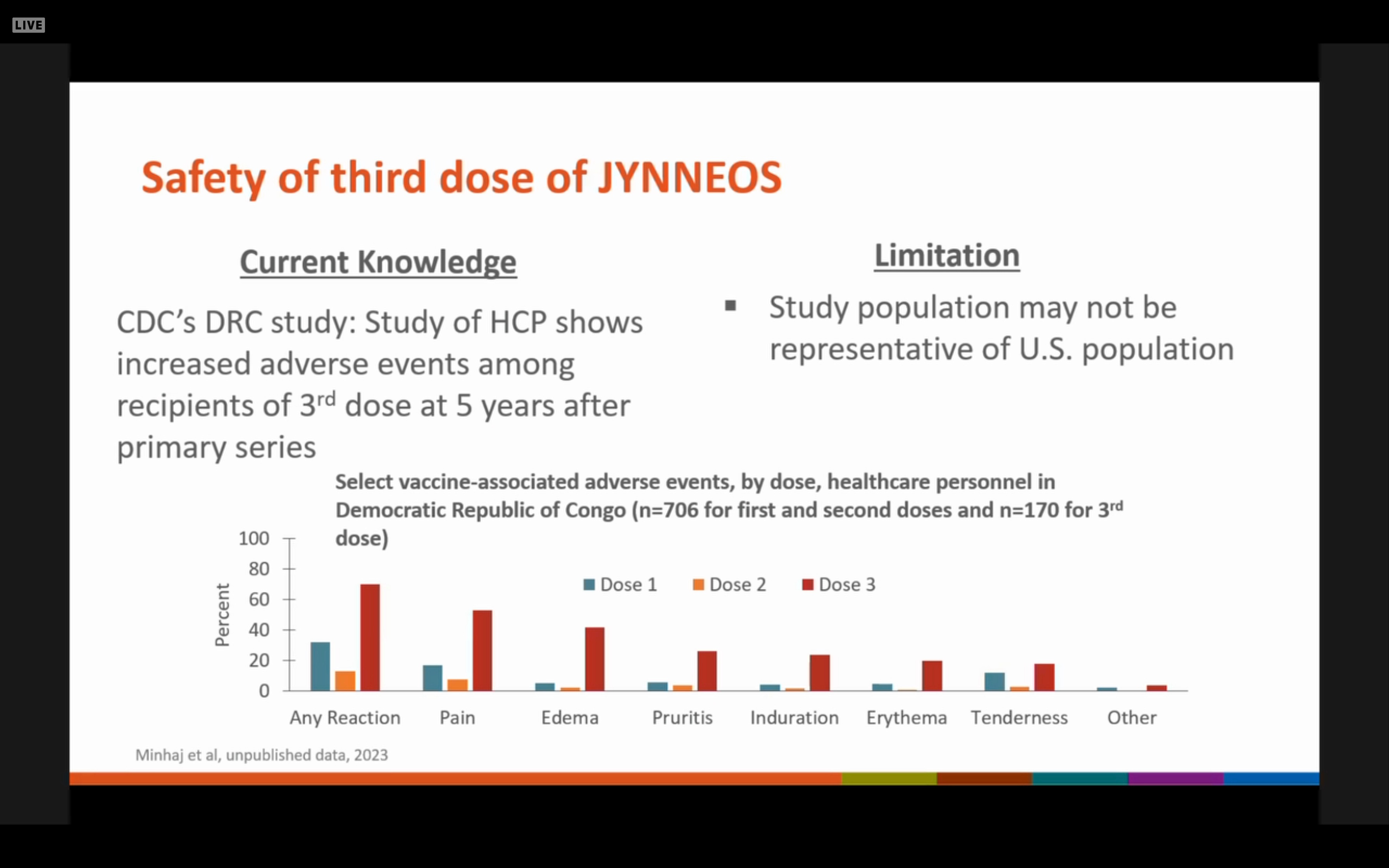
So what did we learn today? After I have beaten CDC up for a year over hiding its 2017 Congo Jynneos trial, today CDC admitted its existence. There were two Congo trials and a total of 1600 subjects.
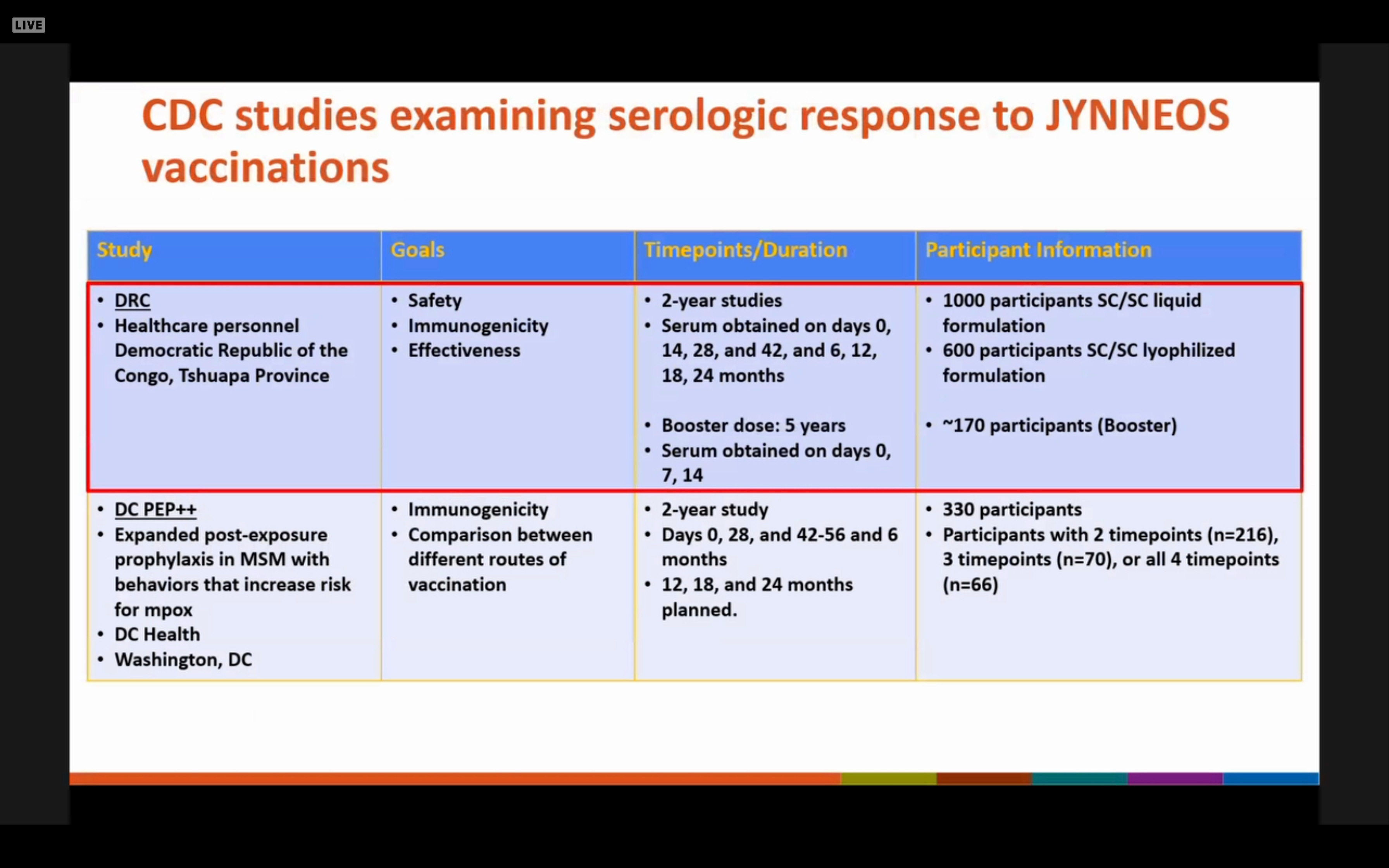
But
CDC’s Dr. Brett Petersen (the Principal Investigator) was nowhere to be
found today. After Dr. Rao mentioned the trials, very little was said
about their findings. No meaningful safety or efficacy information was
presented. Ever heard of a limited hangout? CDC pretended to disclose
but disclosed nothing at all about efficacy. We were told that giving a
3d (booster) dose 5 years after the initial 2 doses caused a lot more
immediate side effects, so probably not a good idea.
The ACIP was also briefed on monkeypox vaccines exactly a year ago today.
But to my knowledge they were never told about the monkey study of
Jynneos. Jynneos had a completely different name at the time—funny how
that happens— and when administered to monkeys it failed to prevent monkeypox in the monkeys.
I
guess it is the depth and consistency of the frauds that get to me.
Everything is either misrepresented , omitted, or an outright lie. As
if it never occurred to CDC officials to tell the truth. What does that
do to someone’s soul? Are the CDC criminals trying to achieve a
certain volume of material injected into all of us, and doing it
piecemeal? Why would they work so hard to push a vaccine that doesn’t
work? Or several?
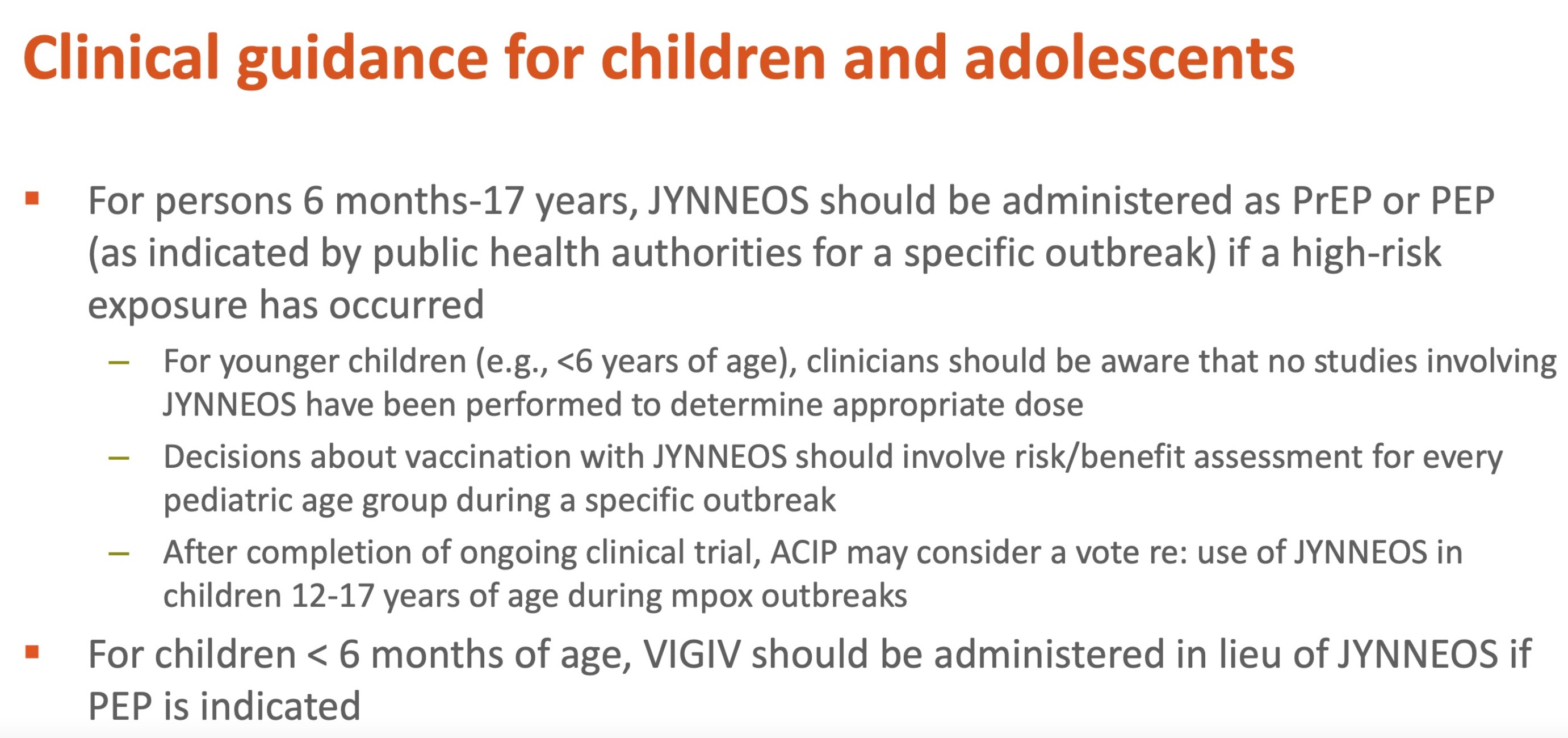
Not only that, they want to expand its use to pregnant women, breastfeeding women and kids. They tried this last year too.

They
also had a similar proposed guidance for kids. But then one of the
ACIP members piped up regarding the fact the vaccine is not licensed for
kids. Uh oh. Then the members realized CDC was trying to inveigle
them into pushing an unlicensed use of the vaccine. Not so fast, CDC.
But these criminals have already given the vaccine to 700 children.
They now think they got the pediatric dose wrong. Whatever that
implies.
There
is a small outbreak going on in Chicago now, and most of the cases have
been fully vaxxed. And of all the monkeypox cases tracked since ? in
the US, 23% had received 2 doses and 37% had received one dose of
Jynneos. That does not sound like it works to me.
Nonetheless,
CDC says the vaccine is highly effective, 89% in one study, but they
will continue to study efficacy. And data-free, they are now pushing
the story that vaccination reduces severity of illness, which wasn’t
severe to begin with…

On to the proposed 5 valent (pentavalent) Meningococcal vaccine.
This simply combines two vaccines into one. Was either needed? Not
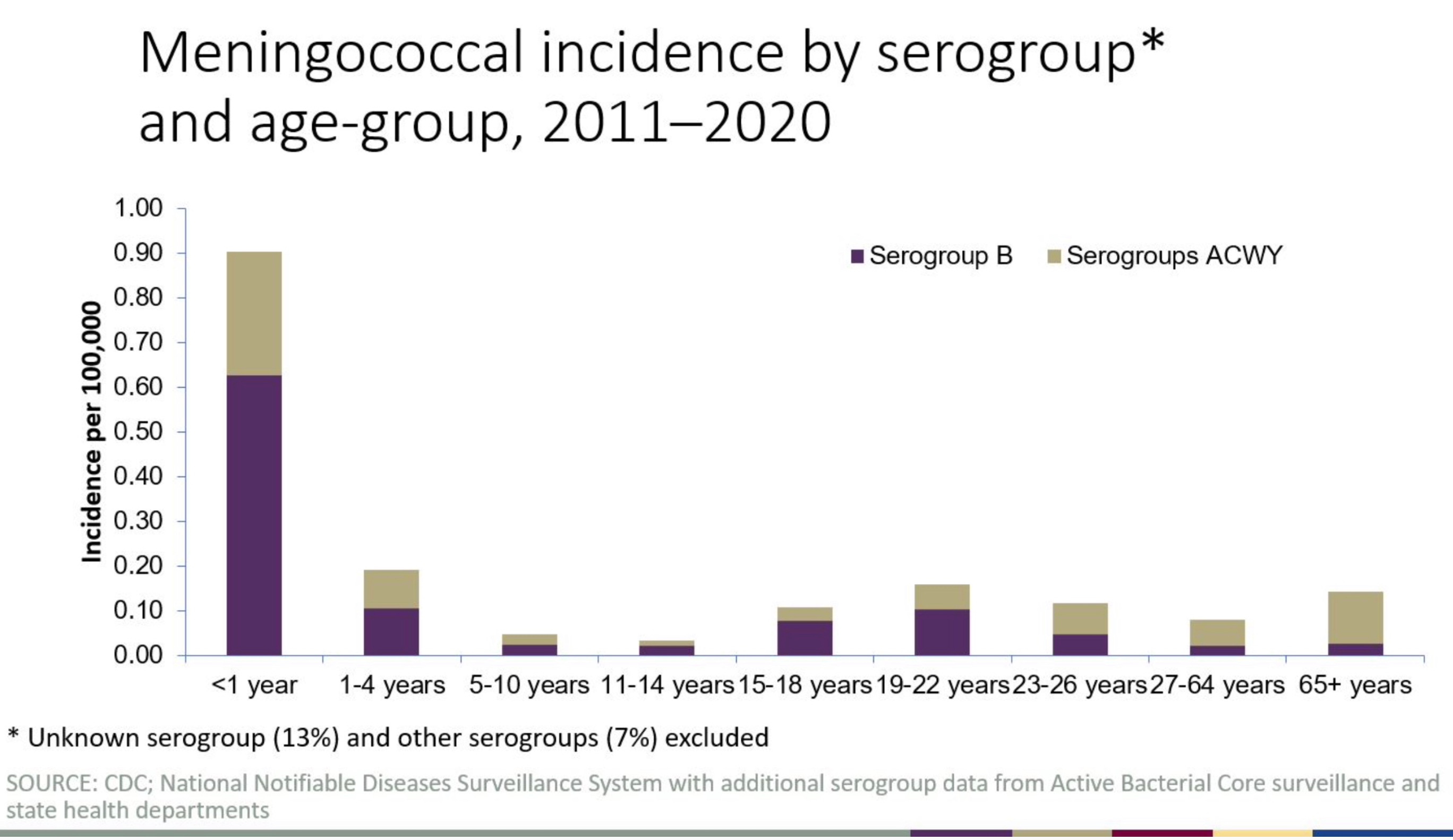
by the 11-14 year age group for whom the Men A vaccine is mandated in
many states. They are at extremely low risk of the disease: about 1 in
30 million per year, according to CDC. The graph below is misleading,
providing the cumulative incidence over a ten year period by age group. For this we vaccinate millions of seventh graders every year. An atrocity.
How long does the vaccine last? We don’t know, probably not long, maybe a couple of years.
I
suspect it was initially recommended for their age group because age 12
was the date for a DTP vaccine booster, so meningococcal vaccine could
be given at the same visit. Of course, 12 year olds did not need a
tetanus or diphtheria booster at that age, since their 5 earlier doses
would be more than adequate. The 12 year pertussis booster would only
work for about two years, and might lead to negative efficacy after
that. I base this on data published about 10 years ago by Nicola Klein
after California instituted the 12 year booster, and then there was a
pertussis outbreak, providing a natural experiment whose results she was
able to catalogue.
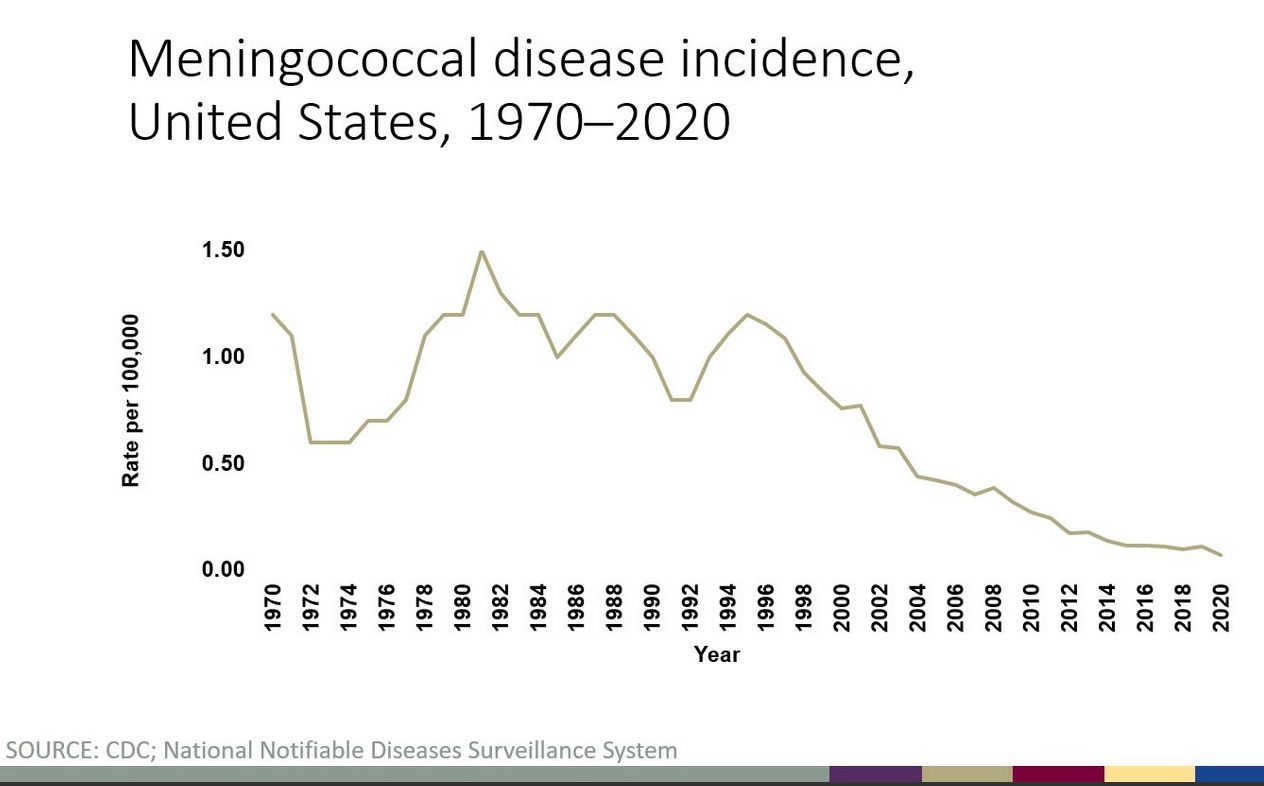
Since this vaccine is not needed, CDC gave us
modelling in lieu of real data to work with. Even that didn’t make the
quadrivalent A, the B or the combined vaccine look very useful. The
meningococcal disease incidence was dropping for unknown reasons for ten
years before the vaccine was introduced in 2005. It kept dropping to
less than one in a million Americans yearly, and the vaccines may or may
not have something to do with that.
There was no discussion of safety
of the Men A or B vaccines, despite the fact that 89% of adolescents
get Men A vax and 31% get the first Men B vax. Only 12% of kids go back
for the second Men B dose! The side effects are therefore probably
severe for the Men B shot.
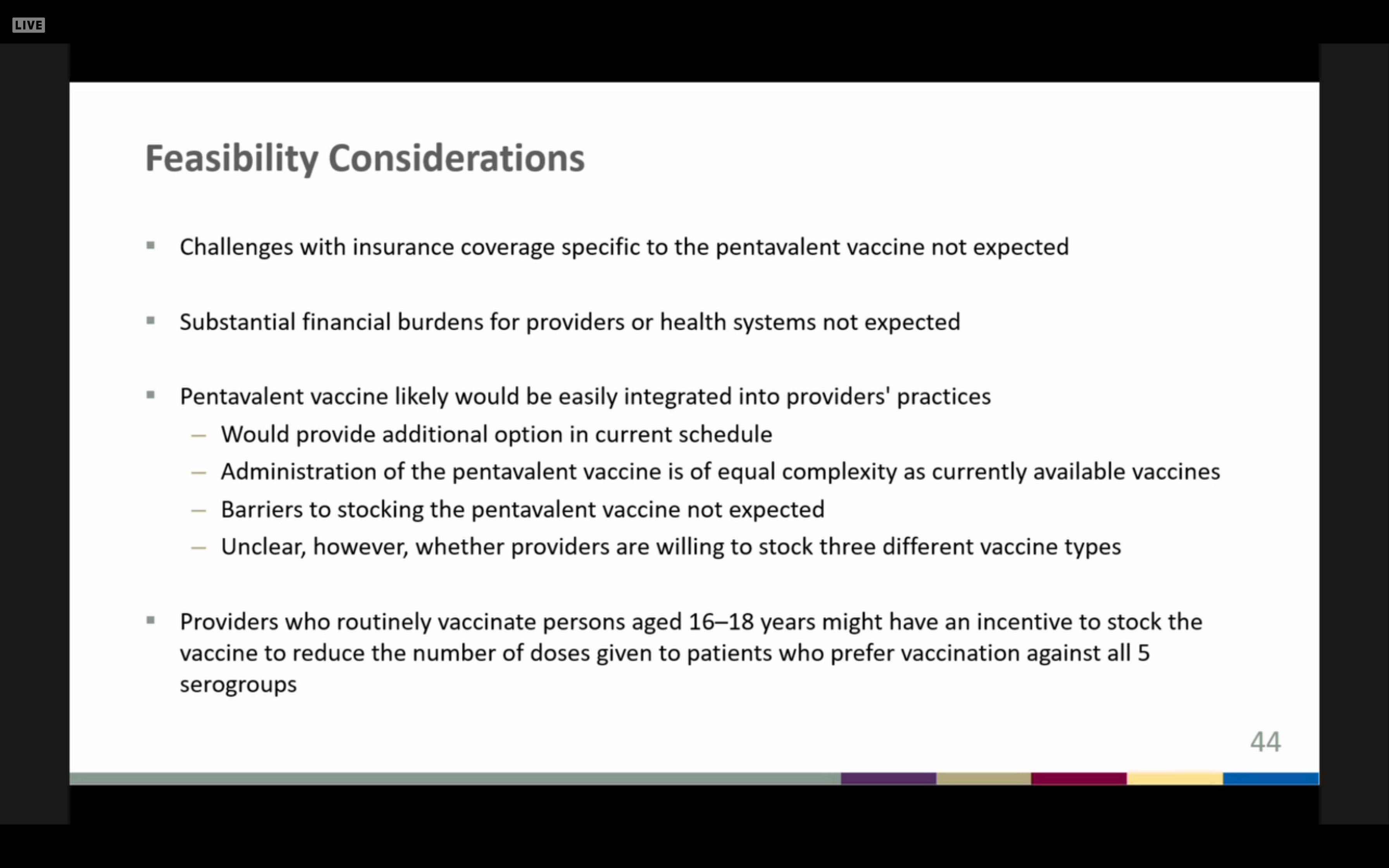
The ACIP members seemed
inordinately concerned about vaccine reimbursements but ridiculously
unconcerned about vaccine costs, or safety. This slide was meant to
soothe them.
Studying the safety of the entire vaccine schedule
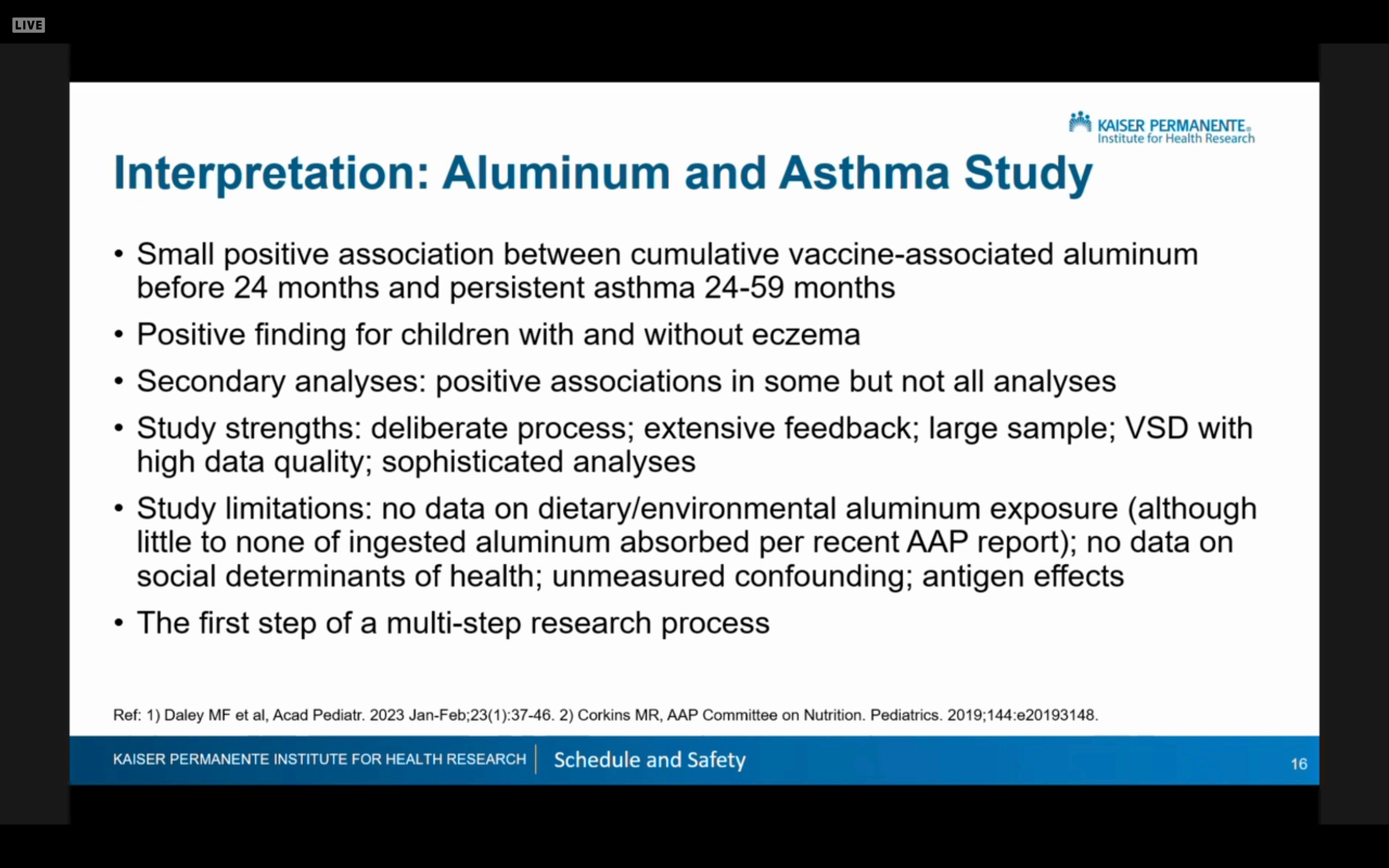
After
this, the committee was presented with very limited studies from the
VSD and medical records companies that alleged to investigate the entire
vaccine schedule’s aluminum burden against the outcomes of diabetes,
asthma and eczema. As expected, the vaccine schedule had nothing to do
with diabetes, but there was a “small positive association” with asthma
and eczema.
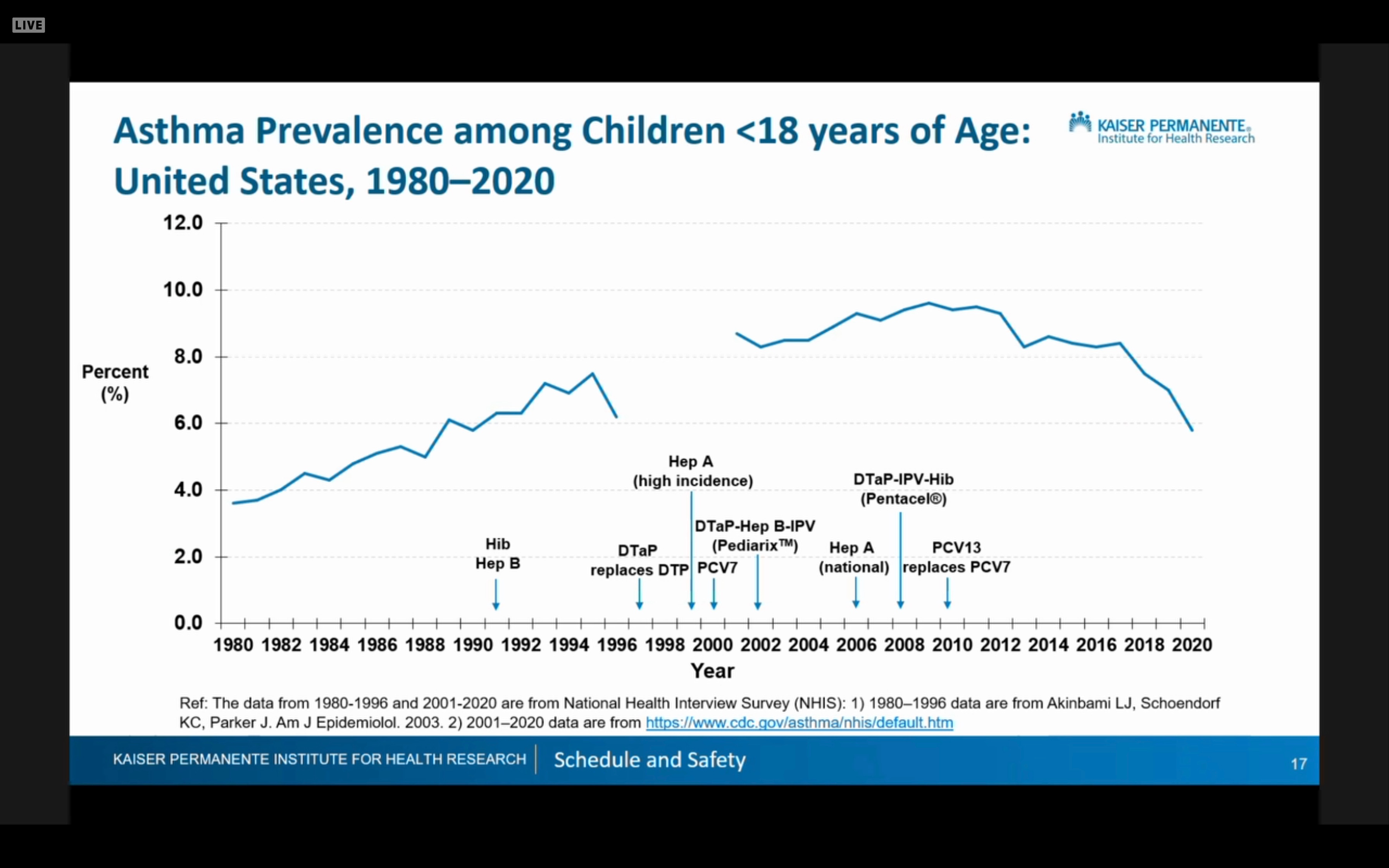
I
thought this was an interesting slide that purported to show asthma
rates are dropping despite more vaccines being added to the schedule.
This shows when vaccines were added recently
One
member picked up a good tidbit that I had missed. The EPIC study
claimed to include 173 million subjects. Hello? Turns out that 173
million Americans have their medical records on software belonging to
the EPIC medical records company. Did they know that EPIC was selling
their data to the CDC? The same turned out to be true for other medical
records companies.
The final act of this 4 ring circus was an attempt to show that the COVID bivalent booster is wonderfully effective and safe, even in pregnancy. And hybrid immunity is the best thing since sliced bread.
But
the claims about hybrid immunity are almost certainly a lie, since very
strong data from the Cleveland Clinic shows the reverse—vaccination
actually detracts from natural immunity.

CDC
went through a song and dance to convince us that Omicron is terribly
dangerous for pregnancy and young babies, and rolled out some data to
convince us that the vaccines were effective for both, despite CDC data
showing waning almost immediately and limited effectiveness in babies
whose moms were vaccinated during pregnancy. Fatuous Sara Oliver (the
Melinda Wharton/Amanda Cohn-in-waiting, an ignorant MD whose job is to
shepherd these meetings along) jumped in and said that while some of
the numbers might not look good, you had to “look at all the data
together” and then you would realize things were pretty good after all.
BTW, only 23% of pregnant moms took a covid shot per CDC—so they
are wising up. But CDC has its eyes on the little kids. After
claiming that hospitalizations were very high in the 6-24 month old
group, it was revealed that CDC is planning a 2 shot initial series for
kids and yearly boosters.
Just say no.