Yesterday’s CDC kerfuffle is not going away. Pulling the wool over the eyes of its expert committee is having deep ramifications. New Committee to review COVID vaccines has been established.
CDC employees whine that they are not being adequately protected after shooting -- what about the public who are not being protected by CDC's criminal commissions and omissions?
Note that the two trials that were incorrectly represented to support the addition of Clesrovimab to the childhood schedule in June were named “Clever” and “Smart.” They don’t look so clever now, however.
Robert Malone has written about how the wool was pulled over his eyes by CDC briefers, noting that the committee only received their briefing booklet the day before the meeting and did not have time to go through the extensive materials carefully.
Clesrovimab sells for $550.00 per dose and was intended to compete with Nirsevimab for market share. It was to be administered to newborns to prevent RSV, which causes many infant hospitalizations but very few deaths (17 per year over a recent 12 year period, according to a CDC review of all US death certificates).
I laid out this sad story when the ACIP approved Nirsevimab 2 years ago for RSV here.
There are 4 million newborns per year in the US. The RSV monoclonal antibody market could be $2.2 billion/year in the US alone
Why did it suddenly become so important to start identifying RSV as a dire threat to newborns and elders? Because NIH (Fauci’s division, naturally) invented an antigen that could be used to make an RSV vaccine and monoclonal antibody, and for every dose sold, NIH and its scientists would receive royalties. So now there are about 5-6 RSV products.
Fauci’s motto: “Build it and they will come.” If you dangle $2 billion a year in front of Big Pharma and little Pharma, and control the FDA’s licensing and CDC’s additions to the childhood schedule, of course they will come. And license what Fauci’s factory invents.
When the 7 ACIP members met in June they were given a skimpy briefing on Clesrovimab and an update on Nirsevimab and they were then asked to vote on approving Clesrovimab for the childhood schedule, making the monoclonal eligible for a liability shield and government and private insurance compensation. The vote was 5 in favor, 2 against. Professor Retsef Levi cast one of the NO votes, having looked at more data than had been presented that were not favorable. He asked CDC staff to comment on his findings. They did not. And his fellow committee members essentially ignored what he was trying to tell them.
With this new look at the CDC data presentation, the ACIP is not at all happy with CDC. I think they will give this product another look at the next meeting.
Another thing CDC’s new ACIP committee will be doing is going to give the COVID vaccines a good hard look. A working group has been established for that, with Professor Levi as its chair. Expect fireworks.
Here is their remit.
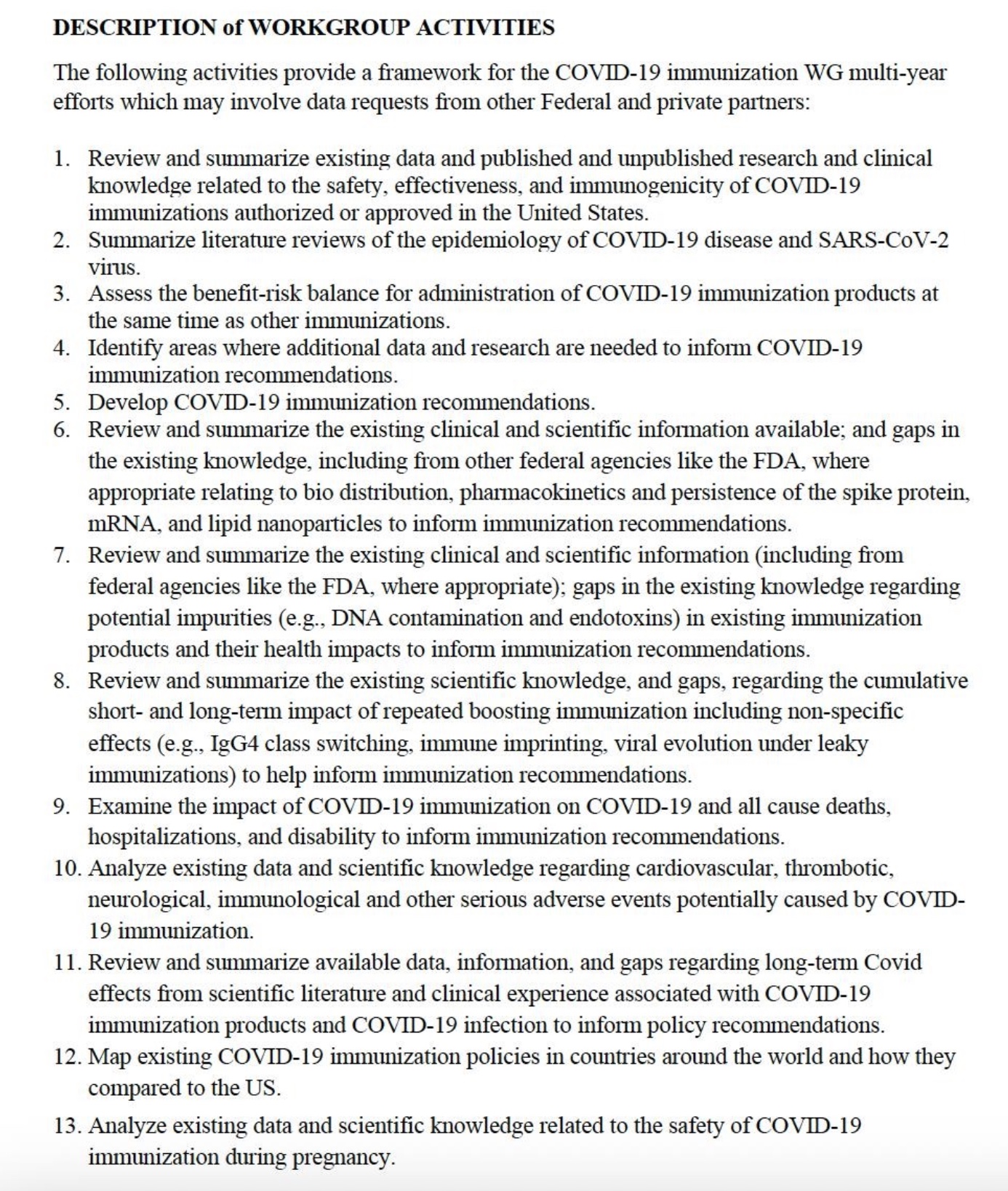
Finally, progress on the COVID vaccine front and uncovering the CDC’s criminality.